Abstract
Diabetes complicates a significant proportion of pregnancies, with gestational diabetes mellitus (GDM) posing a considerable health concern. While the incidence of GDM is rising, its implications extend beyond pregnancy, affecting both maternal and fetal health. Notably, diabetic retinopathy (DR) presents a substantial risk, particularly in women with pre-existing diabetes. However, there remains a dearth of data on retinal vascular changes in pregnant women with GDM managed with medication, particularly in the South Indian population. This study aims to address this gap by evaluating retinal vascular changes in pregnant women with GDM managed with medication, focusing specifically on GDM type A2. We conducted a comprehensive assessment of retinopathy prevalence and associated factors in this population, employing various imaging modalities including fundus photography, optical coherence tomography angiography and Doppler sonography.
Keywords: Diabetes, gestational diabetes mellitus, diabetic retinopathy, retinal vascular
Diabetes in pregnancy, gestational diabetes or pre-existing diabetes, complicates up to 5% of all pregnancies.1 Gestational diabetes mellitus (GDM) is defined as any degree of glucose intolerance developing or first detected during pregnancy.2 GDM can be classified as GDMA1 and GDMA2 by White’s classification system. Gestational diabetes managed without medication and that is responsive to medical nutritional therapy is diet-controlled gestational diabetes or GDMA1. On the other hand, gestational diabetes managed with medication is GDMA2.
Out of all pregnant women with diabetes, 87.5% have GDM, 7.5% have type 1 diabetes mellitus (T1DM) and 5% have type 2 diabetes mellitus (T2DM).1 The incidence of GDM is on the rise because of higher rates of obesity in the population and more pregnancies occurring in older women.3
Metabolic and cardiovascular complications of hyperglycemia during pregnancy for mother and child are now generally recognized with major implications for public health. Women with GDM are not only at risk of short-term pregnancy adverse effects such as pre-eclampsia, but they also have increased long-term risk of obesity, dyslipidemia and T2DM. Women with history of GDM are at 10 times higher risk of developing T2DM in the 1 year after delivery.4 Defects in insulin secretory response and decreased insulin sensitivity, have been observed in GDM mothers similar to that of T2DM which is a major risk factor for cardiovascular disease (CVD), perhaps through endothelial and small vessel dysfunction.5
Diabetic retinopathy (DR) is a microvascular complication and is the leading cause of blindness in women during childbearing years.6 The prevalence of DR in early pregnancy in T2DM is approximately 14% and for T1DM, the estimates range from 43% to 56%.7,8
Chronic hyperglycemia in overt diabetes leads to vasoconstriction, which reduces the blood flow and increases tissue hypoxia. In pregnancy, the pregnant state itself is a risk factor for progression in addition to duration of diabetes, severity of retinopathy at conception, glycemic control, anemia and coexisting hypertension.6
As the glucose intolerance in GDM in most cases is transient, these women are not generally at risk of developing DR in pregnancy. However, some women with GDM have undiagnosed T2DM; this subgroup may develop DR during or following pregnancy. Retinal vascular imaging is a noninvasive tool to study the small vessel dysfunction in overt diabetes.
Due to lack of data on fundus changes in women with GDM, a few studies9-15 over the last decade have attempted to assess the fundus in women with GDM during pregnancy as well as postpartum using different modalities.
A wide range of retinal vascular changes have been described in GDM women in these studies.9-15 Arterial changes such as narrower arteriolar caliber, reduced fractal dimension and larger arteriolar branching angle have been observed. Changes in veins seen were decreased venular caliber and fractal dimension.9 In contrast, another study showed retinal venular widening in GDM mothers to be associated with 5-year metabolic syndrome.12 Hence, there is no clarity about which venular changes are actually associated with GDM on digital retinal photograph images.
Advanced imaging techniques like optical coherence tomography angiography (OCT-A) have shown reduction in vascular density in superficial capillary layer and increase in density in deep capillary layer in pregnant women including mothers with GDM.10 Doppler sonography has also been used, which found a decreased velocity in central retinal artery and ciliary artery in GDM women.11
On the other hand, a cross-sectional study conducted in UK, studied retina using fundus photographs in GDM women, who were on both diet and insulin and found only 2 patients (1.3%) with a single microaneurysm, thereby questioning the utility of routine retinal screening.15 There is a paucity of data regarding changes in the maternal retinal vasculature during pregnancy specifically in women with GDMA2. This is the first study in South Indian population to evaluate retinal vascular changes and contributing factors in pregnant women with diabetes mellitus with specific focus on GDMA2.
The primary objective of the study was to estimate the proportion of retinopathy in pregnant women with GDMA2. The secondary objective was to assess the factors contributing to retinopathy in pregnant women with GDMA2.
MATERIALS AND METHODS
Sampling Population
Pregnant women with GDMA2 were recruited from the antenatal OPD or antenatal ward of Women and Children Hospital, JIPMER, Pondicherry, India
Sample Size Calculation
Sample size was calculated using OpenEpi software version 3.1. The expected proportion of pregnant women with DR in T2DM is 14% and GDM is 1.3%.15 Assuming the proportion of DR in GDMA2 to be 10%, with absolute precision of 3.5% and confidence level of 90%, the minimum required sample size was 196.
Parameters Assessed
Primary outcome
- Proportion having retinopathy
- Grade of retinopathy
Secondary outcome
- Factors contributing to retinopathy
Statistical Analysis
Continuous variables (age, body mass index [BMI], glucose tolerance test [GTT] values, fasting blood glucose [FBG]/postprandial blood glucose [PPBG]) were analyzed by mean (± SD) or median (IQR) depending on the normality of data. Categorical values (parity, education, socioeconomic status, gestational age at diagnosis of GDM, coexisting medical disorders, antidiabetic drugs) were calculated as proportion.
The primary outcome variables (proportion of retinopathy and grade of retinopathy) were calculated as proportion along with 95% confidence interval. Contributing factors for retinopathy were assessed using Chi-square test (for categorical variables) and Students t-test (for continuous variables). P value <0.05 was taken as statistically significant.
RESULTS
Baseline Characteristics
Age
The age distribution of the study population is shown in Table 1 and Figure 1.
The mean age of the study population was 27 ± 3.97 years.
|
Table 1. Age Distribution
|
|
Age (years)
|
n = 196
|
Percentage (%)
|
|
19-34
|
190
|
96.94
|
|
≥35
|
6
|
3.06
|

Educational status
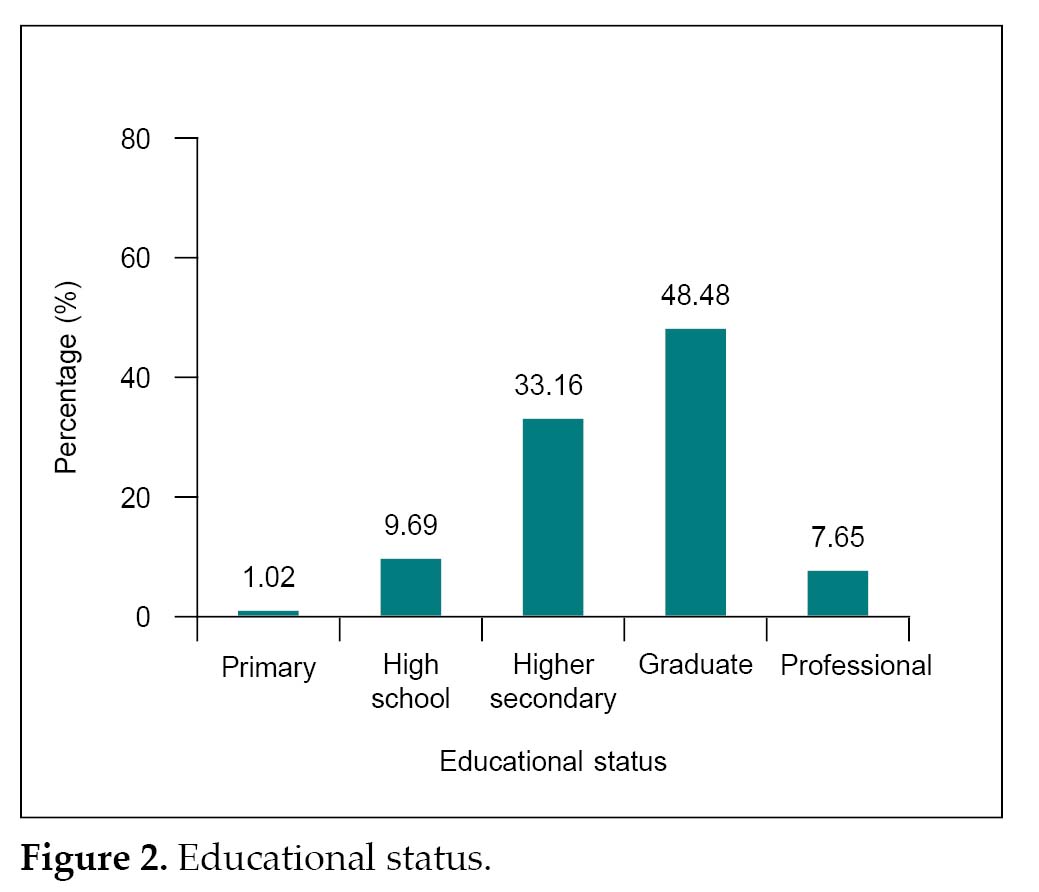
The educational status of the study participants is given below in Table 2 and Figure 2.
Majority of the study population had completed graduation (48.48%) followed by higher secondary schooling (33.16%).
Socioeconomic status
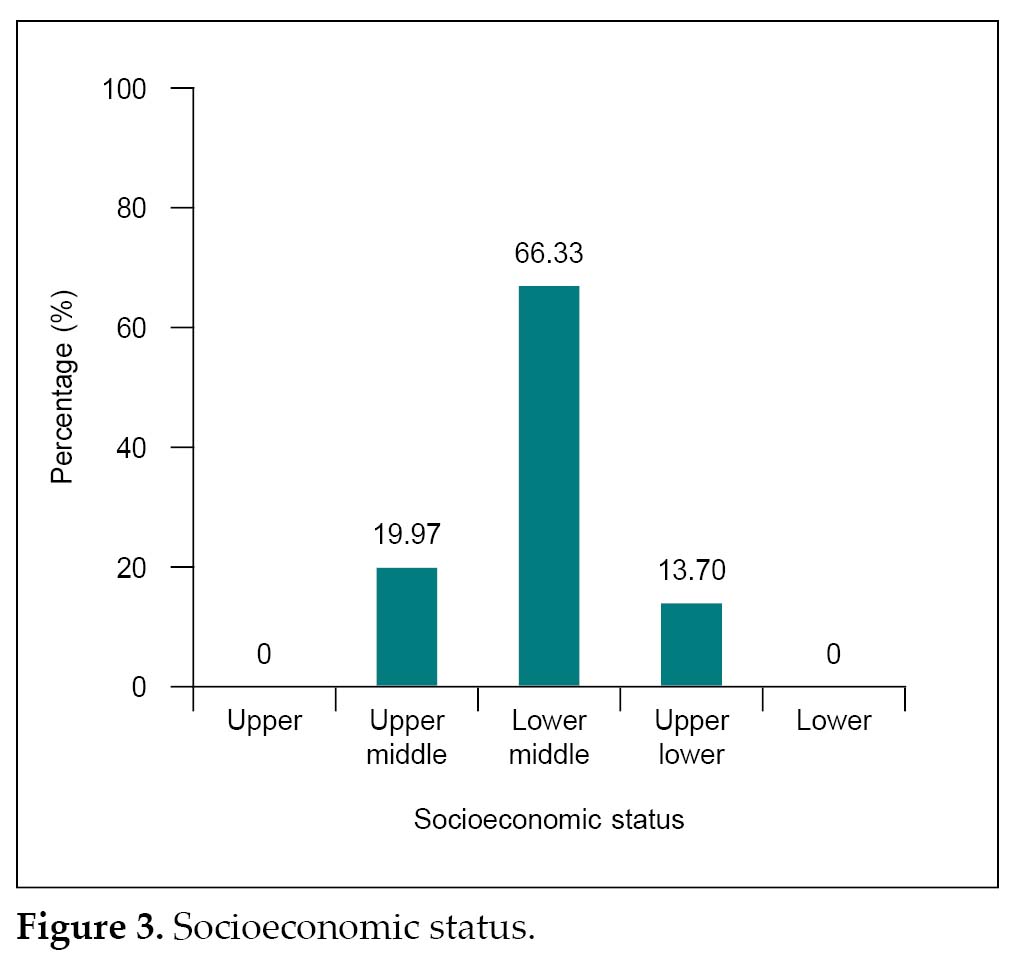
The socioeconomic status of the participants in the study is described in Table 3 and Figure 3.
Most of the women belonged to low socioeconomic status, mainly lower middle class (66.33%).
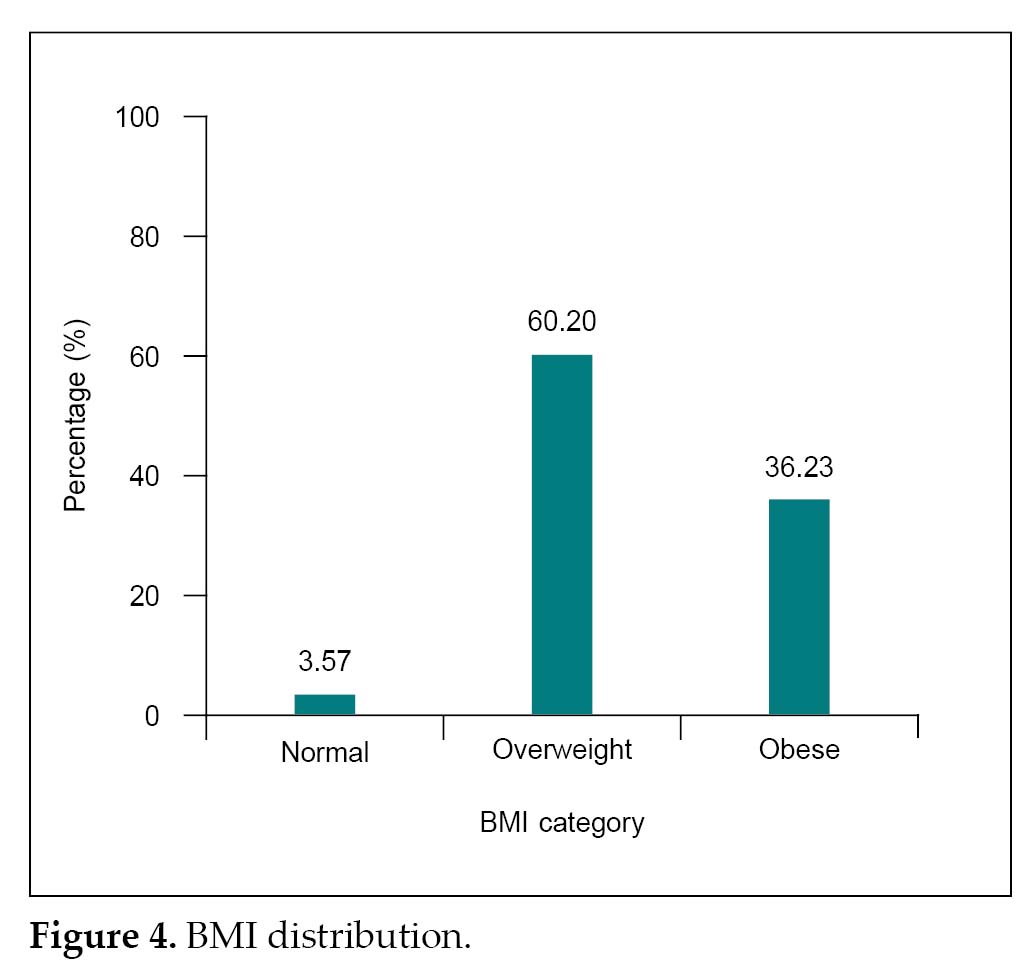
BMI
BMI status of the study participants is shown in Table 4 and Figure 4.
Among the study participants, 60.2% of the women were overweight and 36.23% had obesity.
Obstetric Characteristics
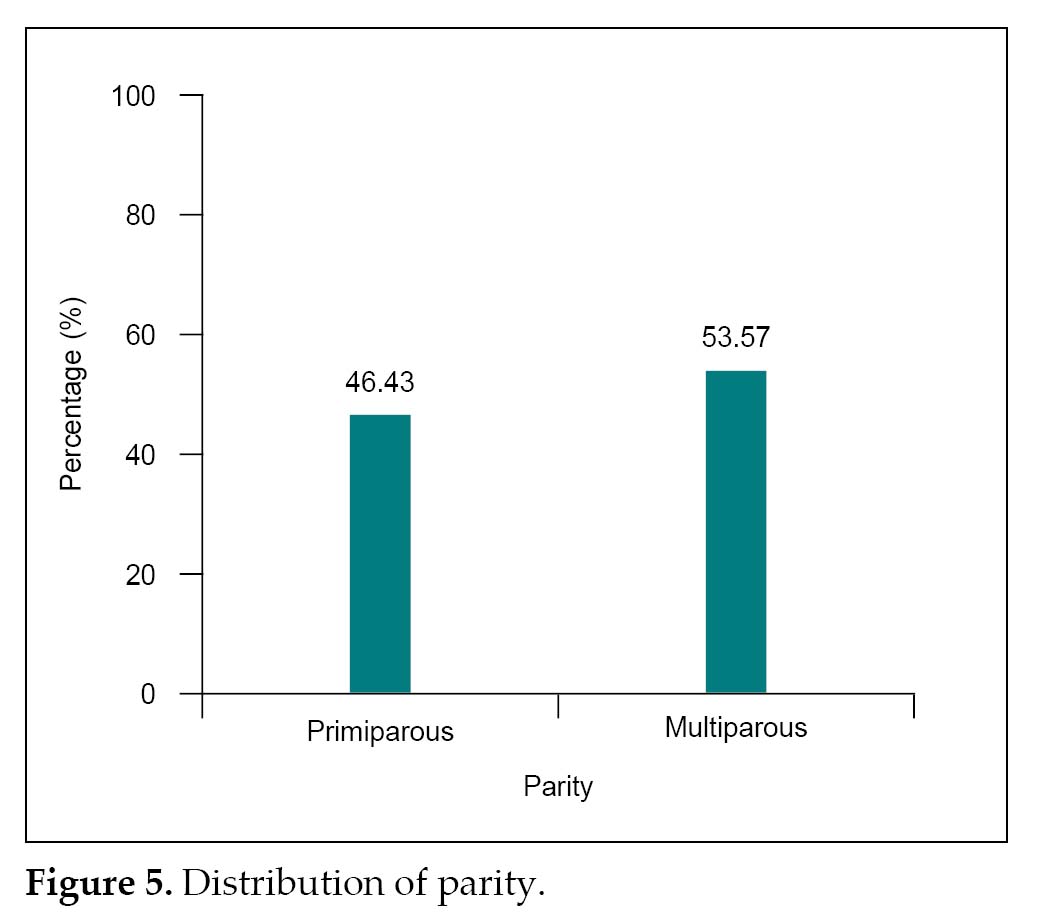
Parity
The parity of the participants in the study is depicted in Table 5 and Figure 5.
There was equal distribution of primiparous and multiparous women amongst the study population.
|
Table 2. Educational Status
|
|
Educational status
|
n = 196
|
Percentage (%)
|
|
Primary
|
2
|
1.02
|
|
High school
|
19
|
9.69
|
|
Higher secondary
|
65
|
33.16
|
|
Graduate
|
95
|
48.48
|
|
Professional
|
15
|
7.65
|
|
Table 3. Socioeconomic Status
|
|
Socioeconomic status
|
n = 196
|
Percentage (%)
|
|
Upper
|
0
|
0
|
|
Upper middle
|
39
|
19.97
|
|
Lower middle
|
130
|
66.33
|
|
Upper lower
|
27
|
13.70
|
|
Lower
|
0
|
0
|
Coexisting medical disorders
Coexisting medical disorders in pregnancy among the study participants are depicted in Table 6.
About 20.41% of women had other medical disorders, mainly hypertension and CVD.
GDM Characteristics
Gestational age at diagnosis of GDM
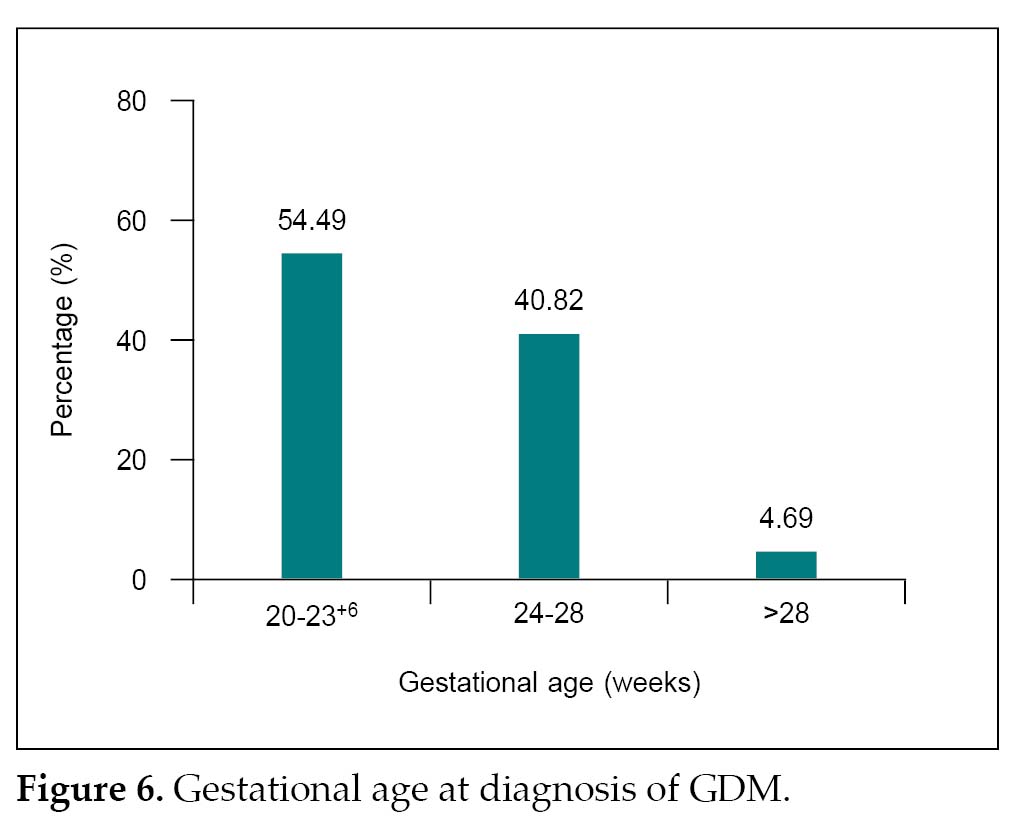
The distribution of study participants based on gestational age at the time of testing 75 g GTT is given in Table 7 and Figure 6.
|
Table 4. BMI Distribution
|
|
BMI category
|
n = 196
|
Percentage (%)
|
|
Normal (18.5- 24.9 kg/m2)
|
7
|
3.57
|
|
Overweight (25-29.9 kg/m2)
|
118
|
60.20
|
|
Obese (≥30 kg/m2)
|
71
|
36.23
|
|
Table 5. Distribution of Parity
|
|
Parity
|
n = 196
|
Percentage (%)
|
|
Primiparous
|
91
|
46.43
|
|
Multiparous
|
105
|
53.57
|
|
Table 6. Coexisting Medical Disorders in Pregnancy
|
|
Medical disorder
|
n = 196
|
Percentage (%)
|
|
Hypertensive disorder of pregnancy (HDP)
|
26
|
13.27
|
|
Cardiovascular disease (CVD)
|
14
|
7.14
|
|
Eye disease
|
0
|
0
|
|
Renal disorders
|
0
|
0
|
|
Table 7. Gestational Age at Diagnosis of GDM
|
|
Gestational age (weeks)
|
n = 196
|
Percentage (%)
|
|
20-23+6
|
107
|
54.49
|
|
24-28
|
80
|
40.82
|
|
>28 weeks
|
9
|
4.69
|
Half of the participants, 54.49% had their 75-g GTT performed at 20-23+6 weeks of gestation, followed by 40.82% who had GTT between 24-28 weeks and another 9 women had GTT after 28 weeks.
GTT values
Distribution of study participants based on the number of abnormal 75 g GTT values is showed in Table 8.
About 2.55% of the patients had one abnormal value, 27.03% had two abnormal values and 70.40% had all three values abnormal on 75 g GTT.
Antidiabetic drugs
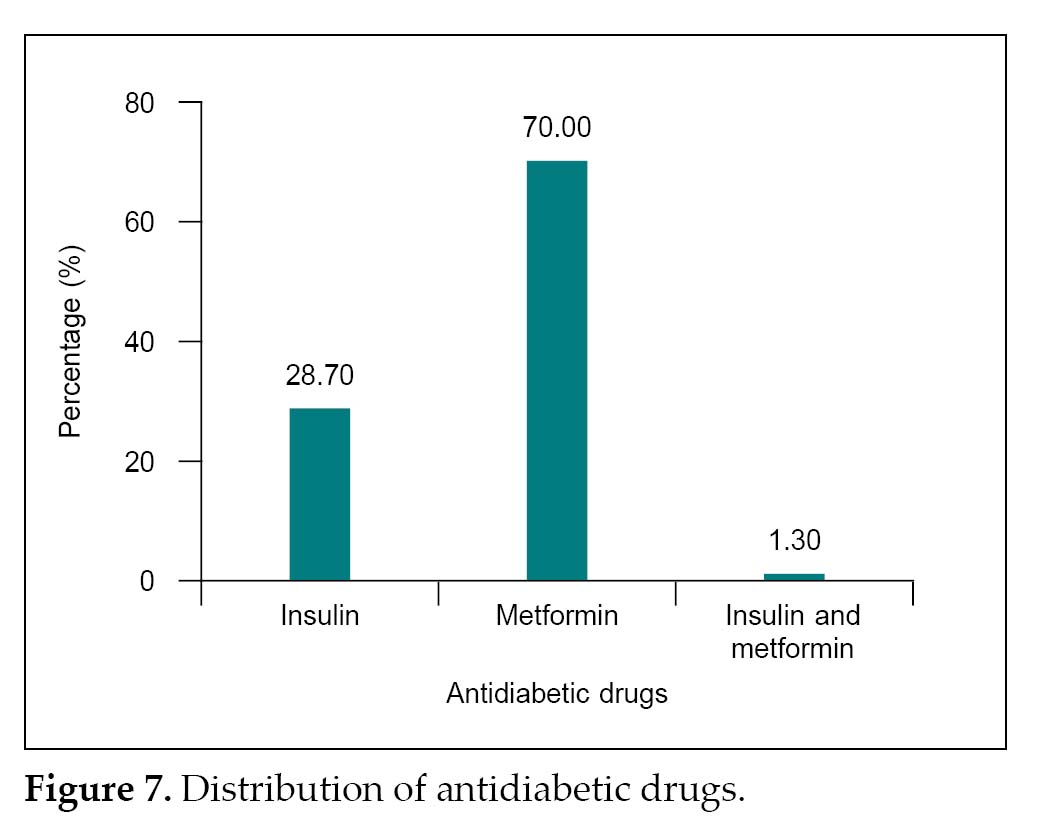
The distribution of different antidiabetic drugs use among study participants is given in Table 9 and Figure 7.
Approximately two-thirds of the women were on metformin therapy in addition to diet and exercise; one-third were on insulin and only 2 patients required combination of insulin and metformin.
Blood sugar profile
Fasting and postprandial blood glucose values are summarized in Tables 10 and 11, respectively.
Around 61% to 63% of study participants had their blood sugar levels within normal range with medication, diet and exercise at the time of fundus examination.
|
Table 8. Distribution of Abnormal GTT Values
|
|
Blood glucose
|
n = 196
|
Percentage (%)
|
|
One abnormal value
Fasting
1 hour
2 hour
|
2
1
2
|
1.02
0.51
1.02
|
|
Two abnormal values
Fasting & 1st hour
Fasting & 2nd hour
1st & 2nd hour
Three abnormal values
|
8
9
36
138
|
4.08
4.59
18.36
70.40
|
|
Table 9. Distribution of Antidiabetic Drugs
|
|
Antidiabetic drugs
|
n = 196
|
Percentage (%)
|
|
Insulin
|
56
|
28.70
|
|
Metformin
|
138
|
70.00
|
|
Insulin and metformin
|
2
|
1.30
|
Retinal Vascular Changes in Pregnant Women with GDMA2
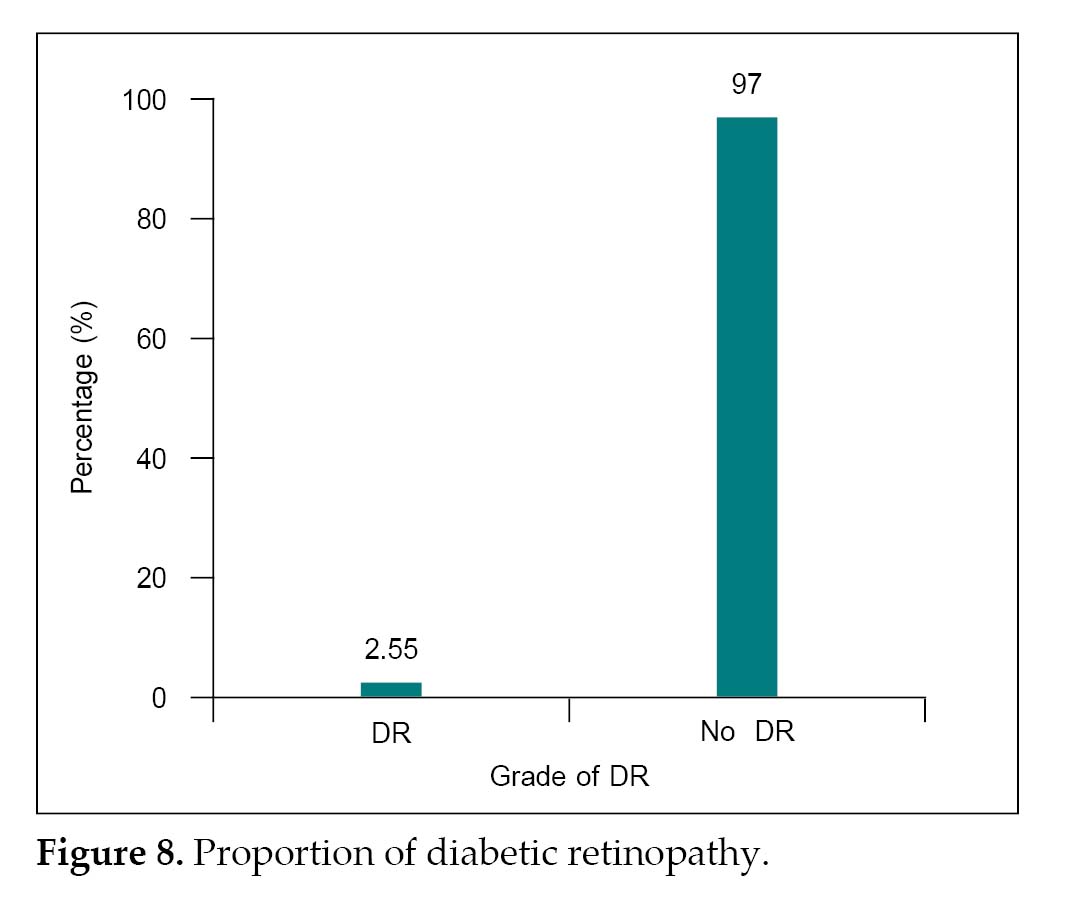
The proportion and grade of DR are shown in Figure 8 and Table 12, respectively.
|
Table 10. Fasting Blood Glucose
|
|
Fasting blood glucose (mg/dL)
|
n = 196
|
Percentage (%)
|
|
<95
|
124
|
63.27
|
|
³95
|
72
|
36.73
|
|
Table 11. Postprandial (2-hour) Blood Glucose
|
|
Postprandial blood glucose (2-hour) (mg/dL)
|
n = 196
|
Percentage (%)
|
|
<120
|
120
|
61.22
|
|
³120
|
76
|
38.78
|
Proportion of retinopathy
Five women (2.5%) with GDMA2 had DR.
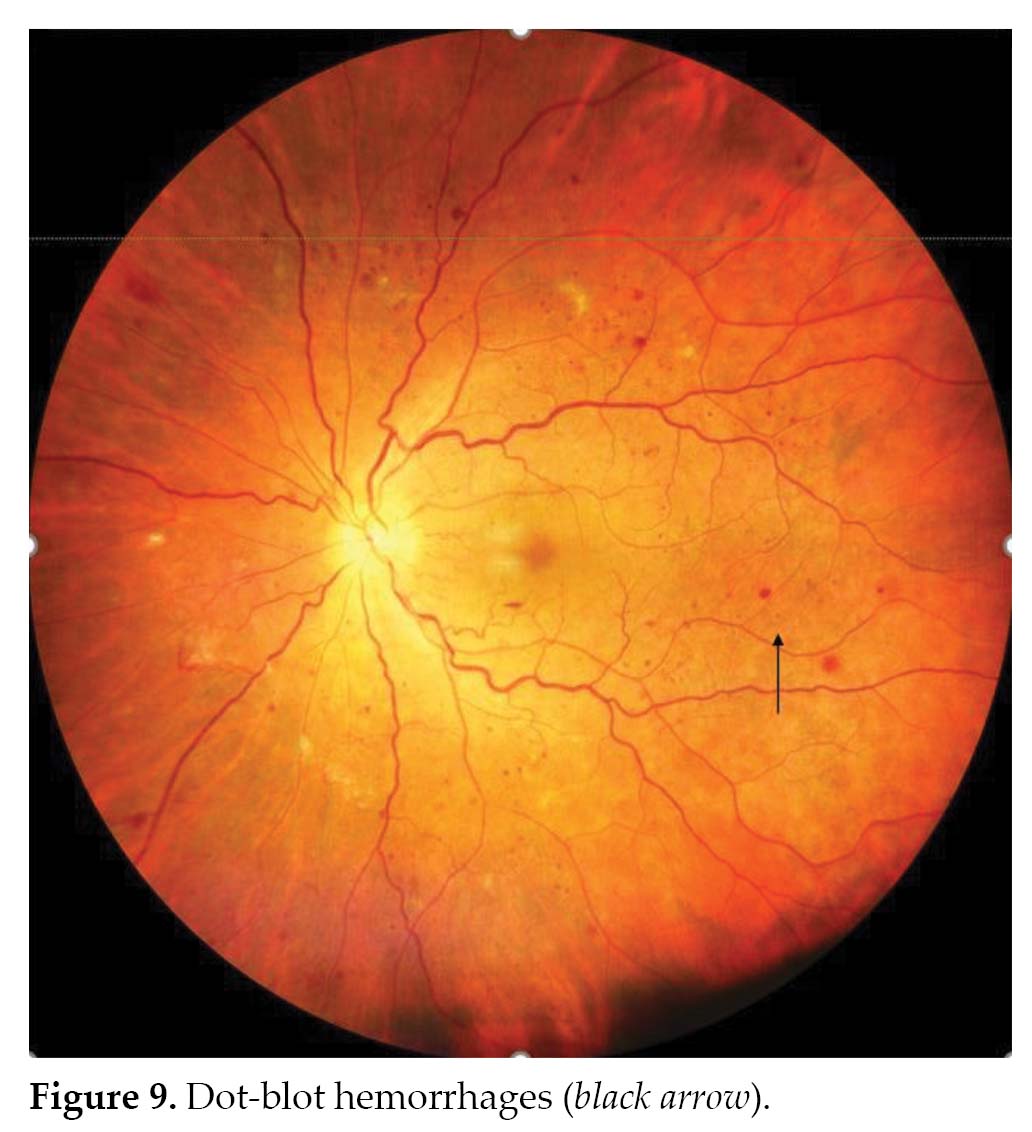
Grade of retinopathy
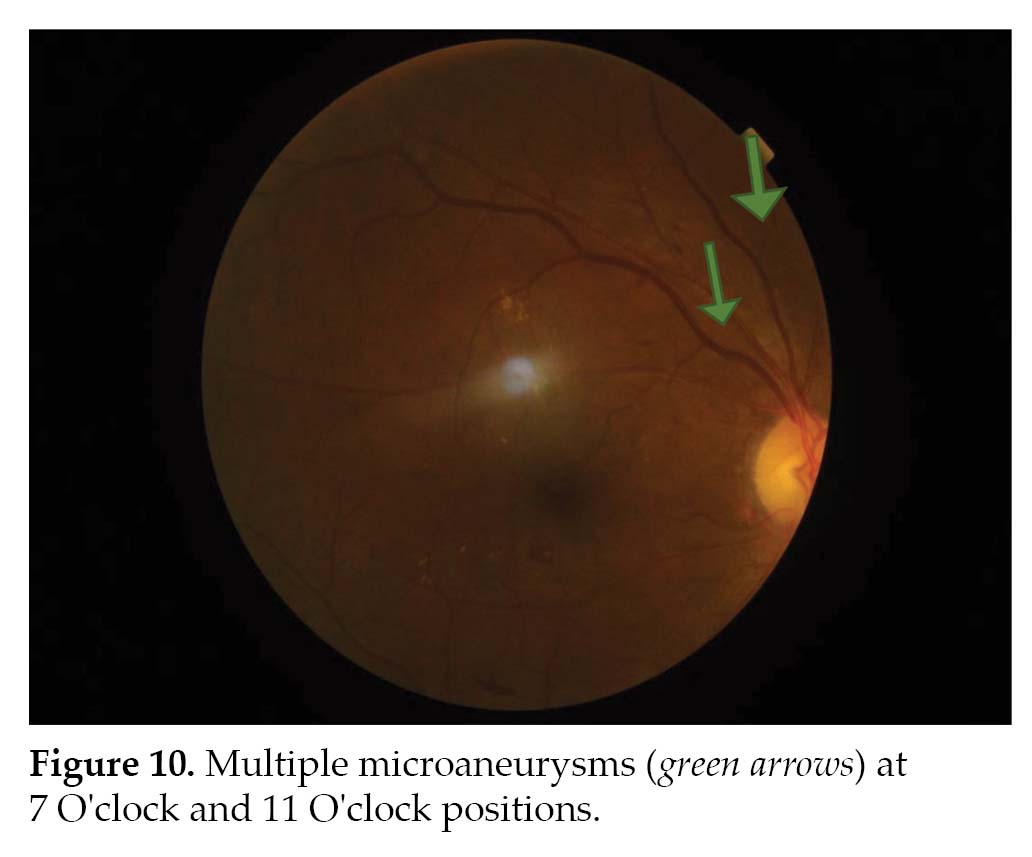
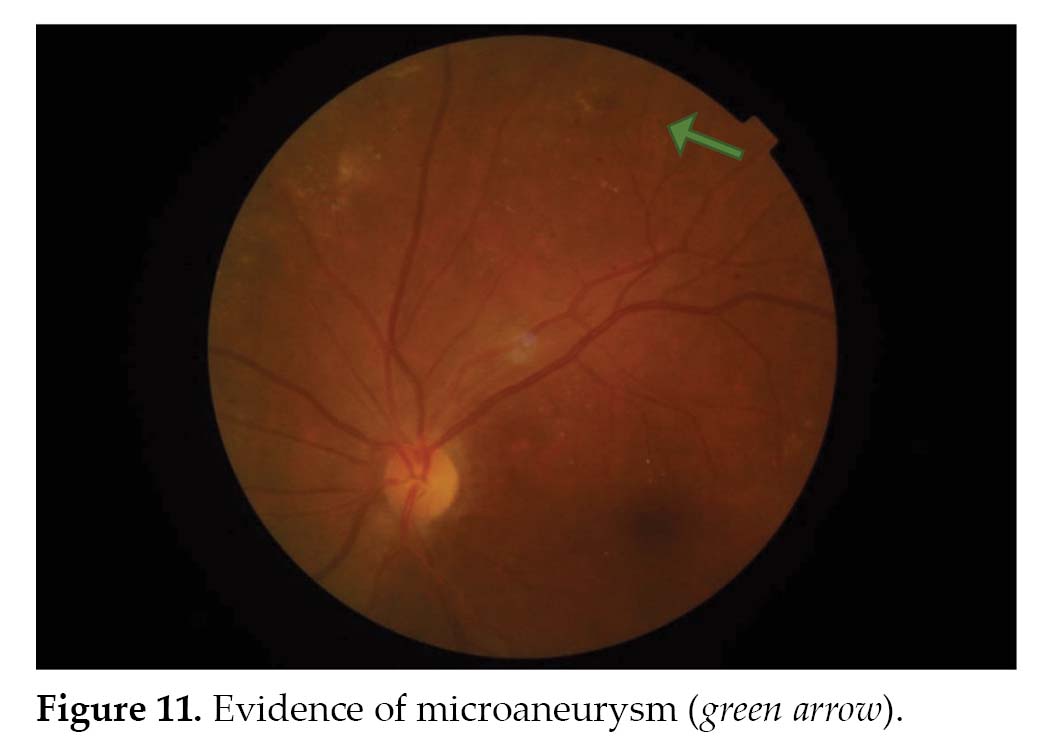
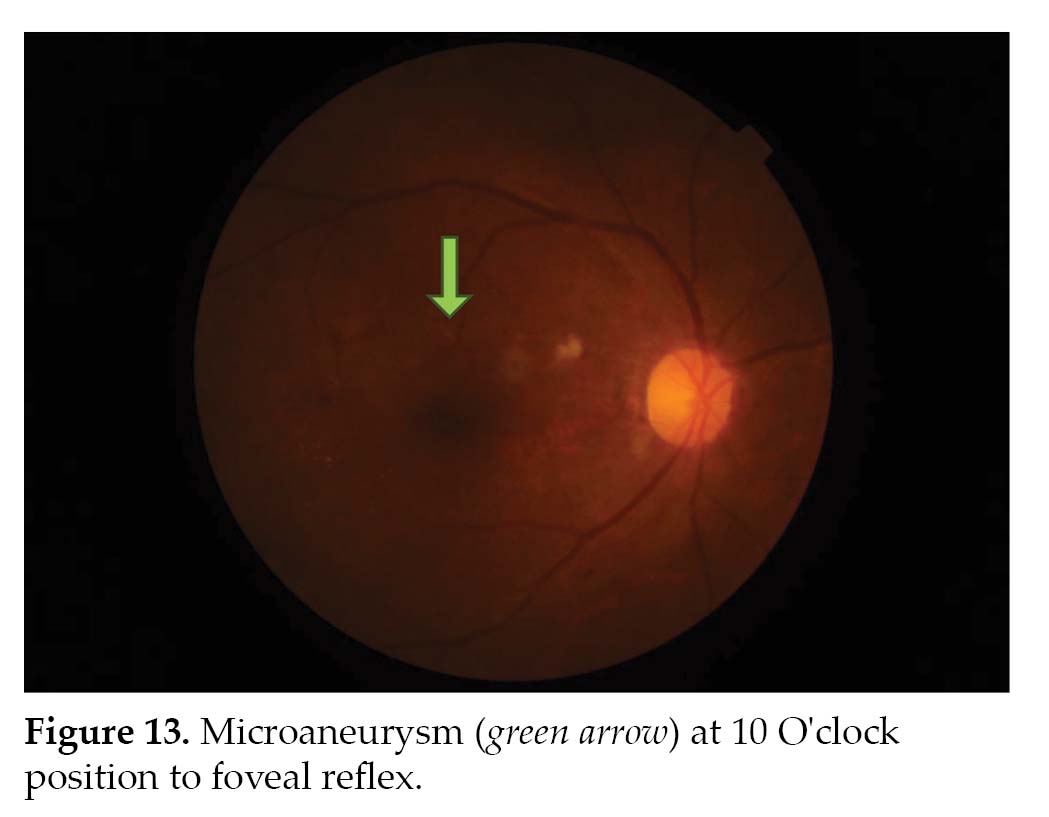
All the 5 women with DR had mild nonproliferative diabetic retinopathy (NPDR) changes and the fundoscopy images in these women are shown in Figures 9-13.
|
Table 12. Grade of Diabetic Retinopathy
|
|
Grade of DR
|
n
|
Percentage (%)
|
|
Stage 2 DR
|
5
|
2.55
|

Other Retinal Vascular Changes
One patient, who had coexisting hypertension along with GDMA2, had Grade 1 hypertensive retinopathy (Keith and Wagner classification) on fundus examination, but no DR changes were observed.
Factors Contributing to Retinal Vascular Changes in Pregnant Women with GDMA2
Factors contributing to retinal vascular changes are shown in Table 13 and Table 14.
There was equal distribution of DR across all age groups. All the cases of DR were found in women with obesity and multiparous women. Significant association was found with respect to parity. One patient with coexisting hypertensive disease had DR changes.
Three women who developed DR were diagnosed with abnormal GTT at 24-28 weeks of gestation. Out of 138 women who had all three abnormal values, 4 had developed DR and 1 woman with 2 abnormal values had DR. Three cases of DR were seen in women who were on insulin and 2 cases were reported in women
|
Table 13. Baseline and Obstetric Factors Contributing to Retinal Vascular Changes
|
|
Characteristics
|
Frequency
|
P value
|
|
Age category (years)
|
|
19-34
|
No DR
DR
|
178
3
|
0.76
|
|
≥35
|
No DR
DR
|
13
2
|
|
BMI
|
|
Overweight
|
No DR
|
7
|
0.663
|
| |
DR
|
0
|
|
Obese
|
No DR
|
184
|
| |
DR
|
5
|
|
Coexisting medical disorders
|
|
HDP
|
No DR
|
25
|
0.653
|
| |
DR
|
1
|
|
CVD
|
No DR
|
14
|
0.53
|
| |
DR
|
0
|
|
Parity
|
|
Nulliparous
|
No DR
|
91
|
0.744
|
| |
DR
|
0
|
|
Multiparous
|
No DR
|
100
|
0.034
|
| |
DR
|
5
|
|
Table 14. GDM Factors Contributing to Retinal Vascular Changes
|
|
Factors
|
|
Frequency
|
P value
|
|
Gestational age at diagnosis of GDM (weeks)
|
|
20-23+6
|
No DR
|
106
|
0.65
|
|
DR
|
1
|
|
24-28
|
No DR
|
77
|
0.88
|
|
DR
|
3
|
|
>28
|
No DR
|
8
|
0.66
|
|
DR
|
1
|
|
GTT values
One abnormal value
|
|
Fasting
|
No DR
|
2
|
0.23
|
|
DR
|
0
|
|
1st hour
|
No DR
|
1
|
0.36
|
|
DR
|
0
|
|
2nd hour
|
No DR
|
2
|
0.27
|
|
DR
|
0
|
|
Two abnormal values
|
|
|
|
Fasting and1st hour
|
No DR
|
8
|
0.56
|
|
DR
|
0
|
|
Fasting and 2nd hour
|
No DR
|
9
|
0.26
|
|
DR
|
0
|
|
1st and 2nd hour
|
No DR
|
35
|
0.38
|
|
DR
|
1
|
|
Three abnormal values
|
No DR
|
134
|
0.30
|
|
DR
|
4
|
|
Antidiabetic drugs
|
|
|
|
Insulin
|
No DR
|
53
|
0.295
|
|
DR
|
3
|
|
Metformin
|
No DR
|
134
|
|
DR
|
2
|
|
Insulin + Metformin
|
No DR
|
2
|
|
DR
|
0
|
|
Blood glucose profile (mg/dL)
|
|
|
|
Fasting glucose ³95
|
No DR
|
71
|
0.43
|
|
DR
|
1
|
|
Postprandial glucose (2-hour) ³120
|
No DR
|
73
|
0.32
|
|
DR
|
3
|
on metformin. No cases of DR were observed in women who were on both insulin and metformin. Three cases of DR were reported in women with uncontrolled postprandial blood sugar compared to one case of DR with uncontrolled fasting blood sugar.
DISCUSSION
Gestational diabetes mellitus with its onset or first recognition during pregnancy is one of the most common pregnancy complications. The prevalence of GDM has considerably increased all over the globe across several racial and ethnic groups. It has been observed that Asian women are at a relatively higher risk of developing GDM even at low BMI cut-offs. We, at a tertiary care center, studied the primary outcomes of proportion and grade of retinopathy in 196 women with GDMA2, and secondary outcome related to the factors contributing to the development of diabetic retinopathy.
Primary Outcomes
Proportion and grade of retinopathy
In our study population, 2.5% of our study participants had mild NPDR on dilated fundus examination. This is similar to a UK based study15 done in 222 women with GDM, which found a prevalence of 1.3% on fundal imaging. However, the participants of this study differed from ours as the 61 women (27.47%) included in their study had GDMA1. Although only microaneurysms were observed in the index study, other changes have been observed in women with GDM in other studies.
Retinal assessment by fundoscopic examination carried out in 88 women with GDM at 26-28 weeks of gestation has shown arteriolar changes, such as narrow caliber, decreased fractal dimension and larger branching angle when compared to non-GDM group suggesting that small vessel dysfunction might be caused by transient hyperglycemia during pregnancy.9 Specifically, larger branching angle present in diabetic women has been linked to atherosclerosis and endothelial damage.6
Preclinical changes of retinopathy have been observed using OCT-A10 including significant reduction of vascular density in superficial capillary layer, but an increased density in deep capillary layer in pregnant women compared to nonpregnant women. In spite of the similar changes in both GDM and non-GDM groups, capillary “dropout” changes in superficial capillary layer were found more in GDM group, but there were no other abnormal microvascular changes pertaining to DR. Also, central macular thinning and foveal avascular zone enlargement was found to be better in GDM mothers when compared to non-GDM mothers.
Apart from fundus imaging and OCT-A, Doppler blood flow of retinal vessels can add further information about microvascular changes such as seen in a cross-sectional study of 65 GDM women of which 10 were GDMA2 and 55 were GDMA1. It was observed that the GDMA2 group had significant reduction of flow velocity in central retinal artery and ciliary artery and higher resistance index in ciliary artery compared to GDMA1.11
However, whether these changes persist after pregnancy and their association with long-term risk of developing T2DM has not been well studied. Addressing this, a prospective cohort study found that second trimester retinal venular widening in digital retinal photographs was associated with a 9.2% incidence of 5-year metabolic syndrome in 142 mothers with GDM independent of the obesity status and maternal sugar control.12 Another study13 used fundus images to study the structure and function of retinal vessels in 127 women with history of GDM at a 5-year follow-up visit. When compared to non-GDM group, they found a reduction in retinal venular dilation in GDM group. This was more significant in women with recurrent GDM than in women who had history of single episode of GDM. A population-based cohort study observed 9,888 women with history of GDM and found more ophthalmic morbidities such as glaucoma, DR and retinal detachment in a mean follow up of 12 years.14
Other retinal vascular changes seen in our study was Grade 1 hypertensive retinopathy in a woman with GDMA2 on insulin with coexisting gestational hypertension although there were no DR changes.
Secondary Outcomes
Factors contributing to retinal vascular changes
Baseline factors
The mean age of our study population was 27 years, which is lesser than the participants in other studies9,10,12,15 in which mean age was above 30 years. The lesser age of our participants could be because of younger age at marriage in Indian population.
Almost half of our study population had completed graduation, which was similar to a study assessing the 5-year incidence of metabolic syndrome in women with GDM.12
However, another study showed a lower proportion of graduates (25%) in their study.9
In our study, we had no patients belonging to the upper socioeconomic class and majority of the study population (66.33%) belonged to lower middle class. Two studies done in Singapore analyzed the socioeconomic status of their study population as a risk factor for retinal vascular changes in GDM women and found that 26% to 30% of them belonged to upper class.9,12 The significance of the socioeconomic status is that obesity is generally prevalent in upper class population, which in turn is a risk factor for diabetes.
Majority of our study population (96%) were either overweight or obese in spite of belonging to lower middle class. This can be attributed to ethnicity of Indian population that predisposes to higher BMI despite low socioeconomic status. In two other studies,9,12 which analyzed BMI as a risk factor for retinal vascular changes; only about 4% of their population were overweight. Higher BMI has been associated with increase in the 5-year incidence of metabolic syndrome in GDM women.12 In contrast, the higher prevalence of obesity in our population was not significantly associated with retinal vascular changes.
Obstetric factors
There was equal distribution of nulliparous and multiparous women similar to one prospective cohort study.12 Nevertheless, all cases of DR (n = 5) were found in multiparous women in our study, out of which, 3 had history of GDM in previous pregnancy, which suggests that recurrent GDM might be a major risk factor for development of DR. This finding of our study is consistent with a prospective cohort study done in Singapore,13 which concluded that women with recurrent GDM had significant reduction in retinal venular vasodilatory response and lower retinal venular dilation (4.5%) when compared to a single episode of GDM.
One-fifth of our study participants had coexisting medical disorders (HDP and CVD). No significant association has been found with coexisting hypertension and GDM associated retinal vascular changes similar to other studies.9,10
GDM factors
In our study, 54% of the study population underwent the 75 g GTT between 20-24 weeks in contrast with all other studies where 75 g GTT was done later at 27-28 weeks.9,11,12,15 It is because of the current practice in India due to high prevalence of GDM to offer testing at 1st visit, 24-28 weeks and 32-34 weeks. There was no significant association of gestational age of diagnosis of GDM with DR.
We analyzed number of abnormal GTT values in our study and found that two-thirds of women had all three values abnormal. We found there was no significant association between these values and the development of DR. Individual GTT values has not been mentioned in the aforementioned studies.9-15 However, higher FBG was proposed to be risk factor for development of 5-year metabolic syndrome in women with history of GDM.12 In our study, the 2 women who had only abnormal FBG did not develop DR, though the number is not high enough to draw a conclusion in this regard.
About 70.4% and 28.7% women in our study on metformin and insulin respectively had developed DR, while the 2 participants taking both metformin and insulin did not develop DR. There was no significant association between the treatment modality and the development of DR (p = 0.29).
Around 62% of study participants had their blood sugar levels within normal range with medication, diet and exercise at the time of fundus examination in our study. There is no mention of blood sugar profile in the other studies except for one study,9 which found no association of FBG with retinal vascular changes. Overall, we found significant association between parity and DR, all 5 women with DR were multiparous (p = 0.034). However, there was no significant association between age, BMI, coexisting medical disorders, gestational age at diagnosis of GDM, number of abnormal GTT values, antidiabetic drugs, blood sugar control at fundus examination and DR in our study. Other studies have not examined the association of these risk factors with retinal vascular changes in women with GDM.9-15
CONCLUSION
This is the first study in South Indian population to evaluate retinal vascular changes and contributing factors in pregnant women with GDMA2 where there is lack of published data. Mild proliferative diabetic retinopathy was seen in 2.5% of pregnant women with gestational diabetes on treatment with either metformin or insulin but not on combination of metformin and insulin. One woman with gestational diabetes on insulin and coexisting gestational hypertension had Grade 1 hypertensive retinopathy with no DR changes.
Multiparity was the only factor significantly contributing to DR. There was no association of age, BMI, 75-g GTT values and glycemic control with DR. Future prospective studies with larger sample size incorporating baseline and frequent assessments will help to understand better about the retinal vascular changes in pregnant women with GDMA2.
REFERENCES
National Collaborating Centre for Women’s and Children’s Health (UK). Diabetes in Pregnancy: Management of Diabetes and Its Complications from Preconception to the Postnatal Period. London: National Institute for Health and Care Excellence (UK); 2015 Feb.
American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2021. Diabetes Care. 2021;44(Suppl 1):S15-S33.
Cunningham F, Leveno KJ, Bloom SL, Dashe JS, Hoffman BL, Casey BM, et al. Williams Obstetrics. 25th Edition. New York: McGraw-Hill; 2019.
Vounzoulaki E, Khunti K, Abner SC, Tan BK, Davies MJ, Gillies CL. Progression to type 2 diabetes in women with a known history of gestational diabetes: systematic review and meta-analysis. BMJ. 2020;369:m1361.
Gabbe S, Niebyl J, Simpson JR, Simpson JE, Jauniaux ERM, Driscoll DA, et al. Obstetrics: Normal and Problem Pregnancies. 1st South Asia Edn-E Book. 1st Edition. Elsevier; 2016.
Schachat AP, Wilkinson CP, Hinton DR, Sadda SR, Wiedemann P (Eds.). Ryan’s Retina E-Book. 6th Edition. Elsevier; 2017.
Rasmussen KL, Laugesen CS, Ringholm L, Vestgaard M, Damm P, Mathiesen ER. Progression of diabetic retinopathy during pregnancy in women with type 2 diabetes. Diabetologia. 2010;53(6):1076-83.
Klemetti MM, Laivuori H, Tikkanen M, Nuutila M, Hiilesmaa V, Teramo K. White’s classification and pregnancy outcome in women with type 1 diabetes: a population-based cohort study. Diabetologia. 2016;59(1):92-100.
Li LJ, Kramer M, Tapp RJ, Man RE, Lek N, Cai S, et al,. Gestational diabetes mellitus and retinal microvasculature. BMC Ophthalmol. 2017;17(1):4.
Liu G, Wang F. Macular vascular changes in pregnant women with gestational diabetes mellitus by optical coherence tomography angiography. BMC Ophthalmol. 2021;21(1):170.
Moneta-Wielgos J, Golebiewska J, Brydak-Godowska J, Ciszewska J, Bomba-Opon DA, Wegrzyn P, et al. Doppler flow parameters in orbital arteries in gestational diabetes mellitus patients. J Matern Fetal Neonatal Med. 2014;27(10):1075-7.
Li LJ, Tan KH, Aris IM, Man REK, Gan ATL, Chong YS, et al. Retinal vasculature and 5-year metabolic syndrome among women with gestational diabetes mellitus. Metabolism. 2018;83:216-24.
Yee KH, Tan KH, Aris IM, Lamoureux EL, Chong YS, Wang JJ, et al. History of gestational diabetes mellitus and postpartum maternal retinal microvascular structure and function. Diabet Med. 2019;36(6):784-6.
Beharier O, Sergienko R, Kessous R, Szaingurten-Solodkin I, Walfisch A, Shusterman E, et al. Gestational diabetes mellitus is a significant risk factor for long-term ophthalmic morbidity. Arch Gynecol Obstet. 2017;295(6):1477-82.
Macfarlane DP, O’Sullivan EP, Dorman S, Allison J, Ellingford A, Pearson ER, et al. The utility of retinal screening in gestational diabetes. Diabet Med. 2013;30(8):
1009-10.
Seshiah V, Balaji V, Shah SN, Joshi S, Das AK, Sahay BK, et al. Diagnosis of gestational diabetes mellitus in the community. J Assoc Physicians India. 2012;60:15-7.